On this page
Cirrhosis is the advanced stage of liver fibrosis, the scarring of tissue that builds up after years of damage. This scar tissue replaces healthy liver, forms nodules, and disrupts both the flow of blood through the organ and its functions. If you have been told you have cirrhosis or chronic liver disease, the most important thing to know is this: cirrhosis does not always advance in a straight line toward liver failure, and we now know that if the cause is treated, fibrosis can stabilize and even regress.
For a long time cirrhosis was considered fixed and irreversible damage. That idea has changed. When the cause is removed or controlled (for example, curing hepatitis C, achieving abstinence from alcohol, or treating fatty liver), many patients improve their liver function and their prognosis. That is why the goal of treatment is not only to manage complications, but to identify the cause and act on it as early as possible.
What is cirrhosis?
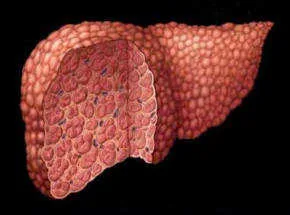
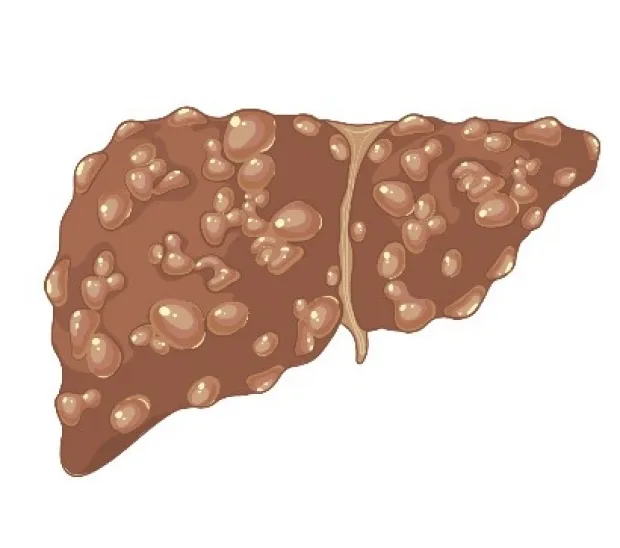
The liver responds to any sustained injury by producing scar tissue, a process called fibrosis. When fibrosis is mild, the liver keeps working well. When it advances and completely distorts the architecture of the organ, with nodules surrounded by scar, we speak of cirrhosis. This scarring obstructs the flow of blood through the liver and raises the pressure in the veins that feed it, a condition known as portal hypertension. Portal hypertension is responsible for many of the complications of cirrhosis.
What causes cirrhosis?
The causes of cirrhosis have shifted over recent decades. Today the most common ones in Chile and worldwide are:
- Fatty liver associated with metabolic dysfunction (MASLD). This is the fastest-growing cause of cirrhosis, tied to obesity, type 2 diabetes, and the metabolic syndrome. It is already the leading cause of cirrhosis in several countries.
- Excessive alcohol use.
- Chronic viral hepatitis: hepatitis C, hepatitis B, and hepatitis D.
Less often, cirrhosis can result from autoimmune diseases such as autoimmune hepatitis and primary biliary cholangitis, from sclerosing cholangitis, from inherited diseases such as hemochromatosis (iron overload) or Wilson’s disease (copper overload), from alpha-1-antitrypsin deficiency, from certain medications, and from chronic congestion due to heart failure. In some cases more than one cause coexists, for example fatty liver and alcohol.
Compensated and decompensated cirrhosis
Not all cirrhosis is the same, and this distinction is what matters most for the prognosis.
- Compensated cirrhosis: the liver, though scarred, still carries out its functions. Most people have no symptoms and many feel well. It is possible to live many years in this phase, especially if the cause is treated.
- Decompensated cirrhosis: this appears when a major complication develops, such as ascites, bleeding from varices, hepatic encephalopathy, or jaundice. It marks a change in the prognosis and calls for closer management.
The aim of treatment is to keep compensated cirrhosis from decompensating and, when decompensation has occurred, to control it. There is also a recognized concept of recompensation: if the cause is removed, some decompensated patients can return to a stable situation, free of ascites and other complications.
What are the symptoms of cirrhosis?
In the compensated phase cirrhosis is usually silent. It can be discovered unexpectedly, on blood tests or an ultrasound ordered for another reason. When they do appear, the first symptoms are nonspecific: fatigue, loss of appetite, general malaise, or weight loss.
The most characteristic signs appear as the disease advances and reflect its complications:
- Jaundice: yellow color of the skin and of the whites of the eyes.
- Ascites: buildup of fluid in the abdomen, which swells.
- Vomiting blood or black stools: from bleeding of the varices in the esophagus or stomach.
- Hepatic encephalopathy: confusion, drowsiness, or behavioral changes, which can progress to coma.
- Itching, a tendency to bruise and bleed, and in men, breast enlargement.
How is it diagnosed and evaluated?
The diagnosis combines the clinical history, the physical examination, blood tests, and imaging. Increasingly, cirrhosis is detected without the need for a biopsy, thanks to noninvasive methods:
- Blood tests: liver enzymes, bilirubin, albumin, and prothrombin time, which reflect liver function, plus the platelet count, which tends to fall in cirrhosis.
- Elastography (for example FibroScan), which measures liver stiffness and estimates the degree of fibrosis and the risk of portal hypertension.
- Abdominal ultrasound, which shows the shape of the liver, the spleen, and the presence of ascites.
Once cirrhosis is confirmed, it is essential to look for and treat the cause, because much of the prognosis depends on it.
Complications of cirrhosis
Almost all serious complications arise from portal hypertension and the loss of liver function:
- Ascites: the most common complication. It is managed by reducing dietary salt and with diuretics; when the fluid is abundant, it is drawn off with a puncture (paracentesis).
- Varices and gastrointestinal bleeding: the esophageal varices can rupture and bleed. They are prevented and treated with beta-blockers and endoscopic band ligation, and in selected cases with a procedure called TIPS.
- Hepatic encephalopathy: the liver stops clearing substances that affect the brain. It is treated with lactulose and, in some cases, rifaximin.
- Jaundice: reflects the decline in liver function.
- Spontaneous bacterial peritonitis: infection of the ascitic fluid, which requires antibiotics and usually calls for ongoing prophylaxis.
- Hepatorenal syndrome: a form of kidney failure that appears in advanced cirrhosis, usually associated with ascites, and that needs hospital treatment.
- Hepatocellular carcinoma: cirrhosis is the main risk factor for liver cancer. For this reason, surveillance with an ultrasound every 6 months is recommended for people with cirrhosis, in order to detect it early, while it is still treatable.
What is the treatment of cirrhosis?
Treatment rests on two pillars.
1. Treat the cause. This is what can halt and even reverse fibrosis:
- In cirrhosis from hepatitis C, direct-acting antivirals cure the infection in the great majority of cases.
- In hepatitis B, antivirals (entecavir, tenofovir) control the virus.
- In alcohol-related cirrhosis, complete abstinence from alcohol is the most effective treatment.
- In fatty liver, weight loss and control of diabetes and cholesterol improve the liver.
- In autoimmune, inherited, or biliary diseases, specific treatments exist.
2. Manage the complications, as described above, and attend to nutrition, avoid unnecessary medications, and keep vaccinations up to date.
When the disease is very advanced and the liver no longer responds, a liver transplant may be the only option and offers excellent results in well-selected patients.
How is the prognosis measured?
To estimate severity and decide the timing of a transplant, two scores are used:
- The Child-Pugh score, which combines bilirubin, albumin, prothrombin, ascites, and encephalopathy.
- The MELD score, based on bilirubin, creatinine, and clotting, used to set priority on the transplant waiting list.
Your physician will use these scores together with the clinical course to guide decisions.
Can you live well with cirrhosis?
Yes, especially in the compensated phase and when the cause is treated. Many people lead a normal life for years. The key lies in timely diagnosis, in eliminating or controlling whatever damaged the liver, and in regular follow-up to prevent and treat complications early.
See also
References
- Ginès P, et al. Liver cirrhosis. Lancet. 2021;398(10308):1359-1376.
- de Franchis R, et al. Baveno VII - Renewing consensus in portal hypertension. J Hepatol. 2022;76(4):959-974.
- Biggins SW, et al. Diagnosis, Evaluation, and Management of Ascites, Spontaneous Bacterial Peritonitis and Hepatorenal Syndrome: 2021 Practice Guidance by the AASLD. Hepatology. 2021;74(2):1014-1048.
- Singal AG, et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78(6):1922-1965.
- Israelsen M, et al. Steatotic liver disease. Lancet. 2024;404(10464):1761-1778.
Related articles
Causes of liver cirrhosis
The causes of cirrhosis, from the most to the least common, and why identifying and treating the cause early can stop and even reverse liver damage.
Hepatology: what it is and what a hepatologist does
Hepatology is the branch of medicine that studies the liver and bile ducts. What a hepatologist does and when you should see one.
Nutrition and the liver: what to eat for your liver condition
How to eat with fatty liver or cirrhosis: Mediterranean diet, how much protein, salt in ascites, and why no food actually cleanses the liver.